Degenerative scoliosis or adult-onset scoliosis is defined as a curvature of the spine of at least 10 degrees.
The more common variety is known as “de novo” scoliosis, and is caused by degeneration of the facet joints and intervertebral discs occurring gradually over a period of time during adulthood. The scoliosis is usually located in the low back or lumbar spine (Figure 1).
The less common variety may begin from the teenage years as adolescent idiopathic scoliosis but may not be diagnosed until later in adulthood. The scoliosis may have curves located at the mid back (thoracic spine), low back (lumbar spine), or both.

Figure 1
Common Symptoms
Contributing Factors to Symptoms
Diagnosis
(i) Medical History
The location of pain as well as the triggering factors are especially important to the doctor to narrow down the cause and source of the pain.
(ii) Physical examination
The posture of the spine will be assessed. The strength, sensation, and reflexes of the legs will also be checked.
(iii) Imaging scans
X-rays
Standing x-rays of the whole spine are done to assess the degree of scoliosis (Figure 2) and kyphosis. Bending x-rays of the low back may also be done to rule out any mal-alignment of the low back.

Figure 2
MRI
MRI provides a closer assessment of any evidence of compression of the nerves, and if there are, what are the offending structures (e.g. discs, bone spurs, thickened ligaments).
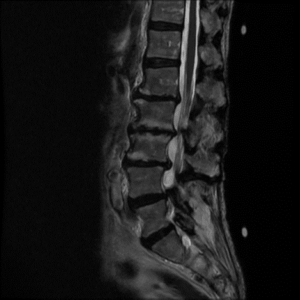
Figure 3(i)
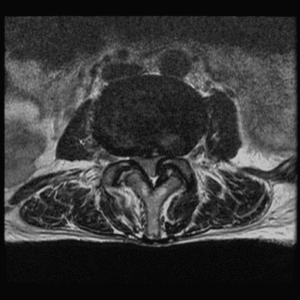
Figure 3(ii)
Treatment
The treatment objective is to reduce pain and/or any neurological symptoms.
Non-Surgical
Spinal Injection
Spinal injections may be offered if the patient does not respond adequately to the above measures. The injections frequently target the facet joints and nerves which are responsible for the symptoms. These injections deliver the anti-inflammatory medications directly to the affected area in the back via x-ray guidance. The procedure is done in the operating room to ensure sterility and access to x-ray imaging facilities.
Surgery
If the pain and/or neurological symptoms continue to significantly affect the quality of life despite undergoing the above-mentioned treatment, surgery may be considered. The recovery time after surgery is significant, ranging from 2 to 12 months, so the symptoms should be severe enough to warrant such a procedure. The objectives of surgery are to preserve the function of the nerves as well as relieve pain and /or neurological symptoms. Sometimes degenerative scoliosis curves can exceed 50 degrees and continue to progress, and this is another indication for surgery, lest there be major spinal balance problems, severe pain, and cardiopulmonary complications.
Decompression surgery is one surgical method. It involves removing the lamina, ligamentum flavum, disc and part of the facet joint, in order to relieve pressure on the nerves. This may be done in a keyhole or minimally invasive fashion thereby reducing damage to the normal tissue structures.
More commonly, the decompression surgery is combined with a fusion. This is often necessary as a decompression alone in the setting of a scoliosis curvature, may potentially cause the spine to become more unstable and cause the scoliosis to worsen. However, decompression surgery without fusion may be recommended for elderly patients with mainly nerve compression symptoms at one level of the spine. Avoiding fusion may speed up the recovery process in such potentially frail patients.
A fusion refers to “joining” the multiple spine segments to create a stable spine. This requires implants of various types to maintain the stability while the bones “join” together. Implants commonly used include cages, screws, and rods. The fusion surgeries are usually done from the back (posterior approach), but in some cases they can be done by going through the front or the side (Figure 4). Sometimes in complex cases, the doctor may stage the surgery into two procedures. That means the doctor will perform the first part of the surgery on day 1 and the second part 3 to 5 days later.

Figure 4
The fusion could be long (span much of the back) or short (fuse only one or two vertebral levels). If scoliosis is severe, a long fusion is often needed in order to stabilize the spine and partially correct the scoliosis (Figures 5). The short fusion could be an option for a more moderate scoliosis, or if the surgical attention is only directed at the segments of the spine that are causing nerve compression.

Figure 5A

Figure 5B