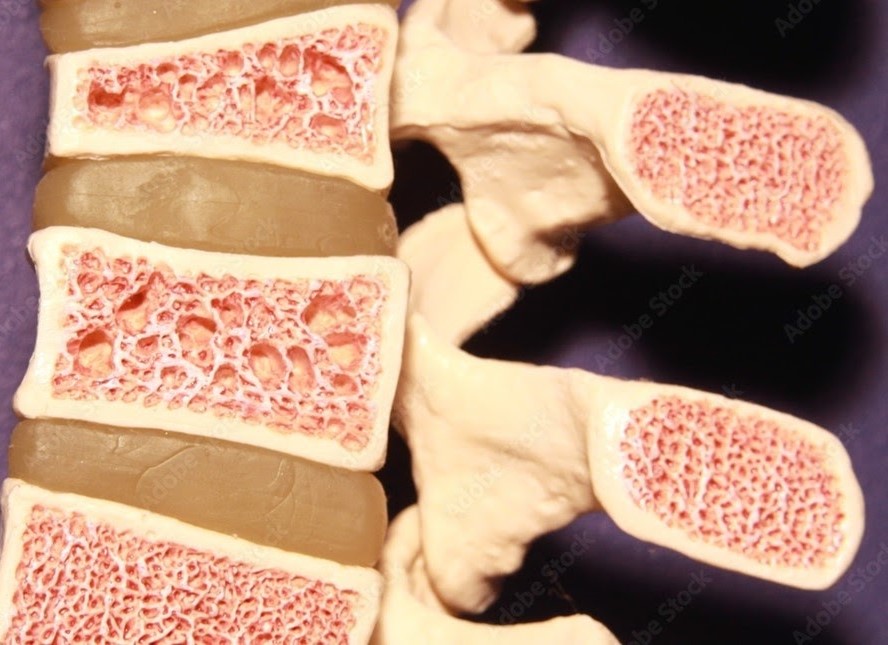
Our bone mass peaks at age 35 and starts to decrease progressively after that. It has been estimated that 90% of the population of women above the age of 75 are clinically osteoporotic.
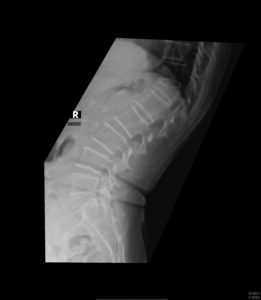
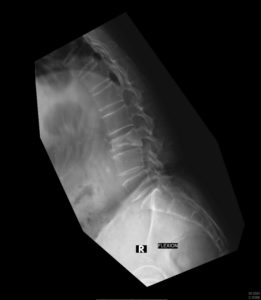
The lifetime risk of a symptomatic osteoporotic fracture has been reported as 16% for females and 5% for males. Fractures of the vertebrae (spine), hips, and distal radius (wrist) are the more commonly encountered fractures related to osteoporosis, with spinal fractures the most commonly seen. The fractures may occur even without a history of fall due to the fragility of the skeleton.
Complications of such fractures include chronic pain, spinal deformity (kyphosis or hunched back), spinal cord compression leading to paralysis/loss of bladder or bowel control, and breathing difficulties. Various studies have shown a 30% increase in mortality upon diagnosis of an osteoporotic spine fracture.
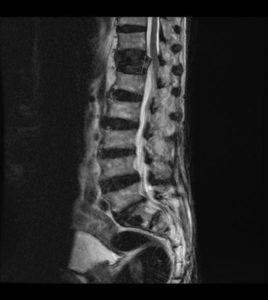
Diagnosis
Investigations
Treatment
(i) Vertebroplasty
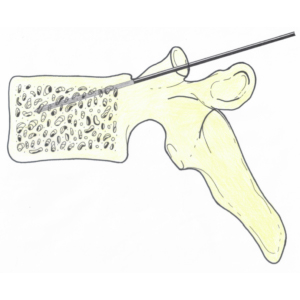
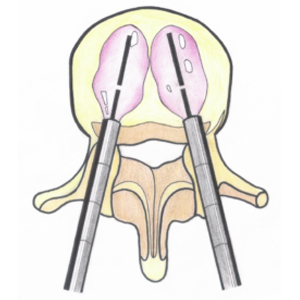
This procedure is a minimally invasive percutaneous (without surgical incision) technique in which the integrity and structure of a damaged or destroyed vertebral body is augmented through the use of bone cements. This procedure has gained widespread acceptance because of its efficacy and ability to be performed under sedation and not general anesthesia, thus allowing it to be performed as a day surgery procedure.
(ii) Kyphoplasty
This procedure is an improved version of vertebroplasty, where an inflatable balloon is inserted in the fractured vertebra to create a void for cement filling (balloon is removed prior to cement injection). This method further raises the safety level of the procedure, as the risk of cement leakage is reduced significantly as compared to vertebroplasty.
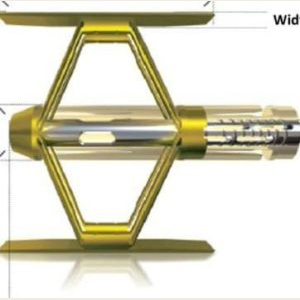
(iii) Stenting
Stenting in the fractured vertebra reinforced by injection of bone cement around it is another modification of the vertebroplasty technique. The stent and the cement help to maintain the integrity of the fractured vertebra.
Apart from managing the osteoporotic spinal fracture, it is important to treat the general osteoporosis condition as well. This can be achieved with various medications. Available options include oral weekly risedronate, six monthly injection of denosumab, daily injection of teriparatide or monthly injection of romosozumab.
Surgery
In severe cases of osteoporotic fractures causing neurological compromise, surgery may be required. This entails decompression of the nerves as well as stabilization of the fractured vertebra via titanium screws inserted above and below the fractured vertebra. Such screws may be reinforced with cement to strengthen the purchase of the screws into the vertebrae, preventing implant failure.

